



A major new review suggests the new generation of obesity drugs can deliver striking weight loss, but their wider benefits remain uneven. For travel and tourism, that nuance matters: the rise of GLP-1 medicines may reshape traveller behaviour, medical tourism, hospitality demand, and accessibility expectations, but it is unlikely to be a simple story of lighter passengers and healthier holidays.
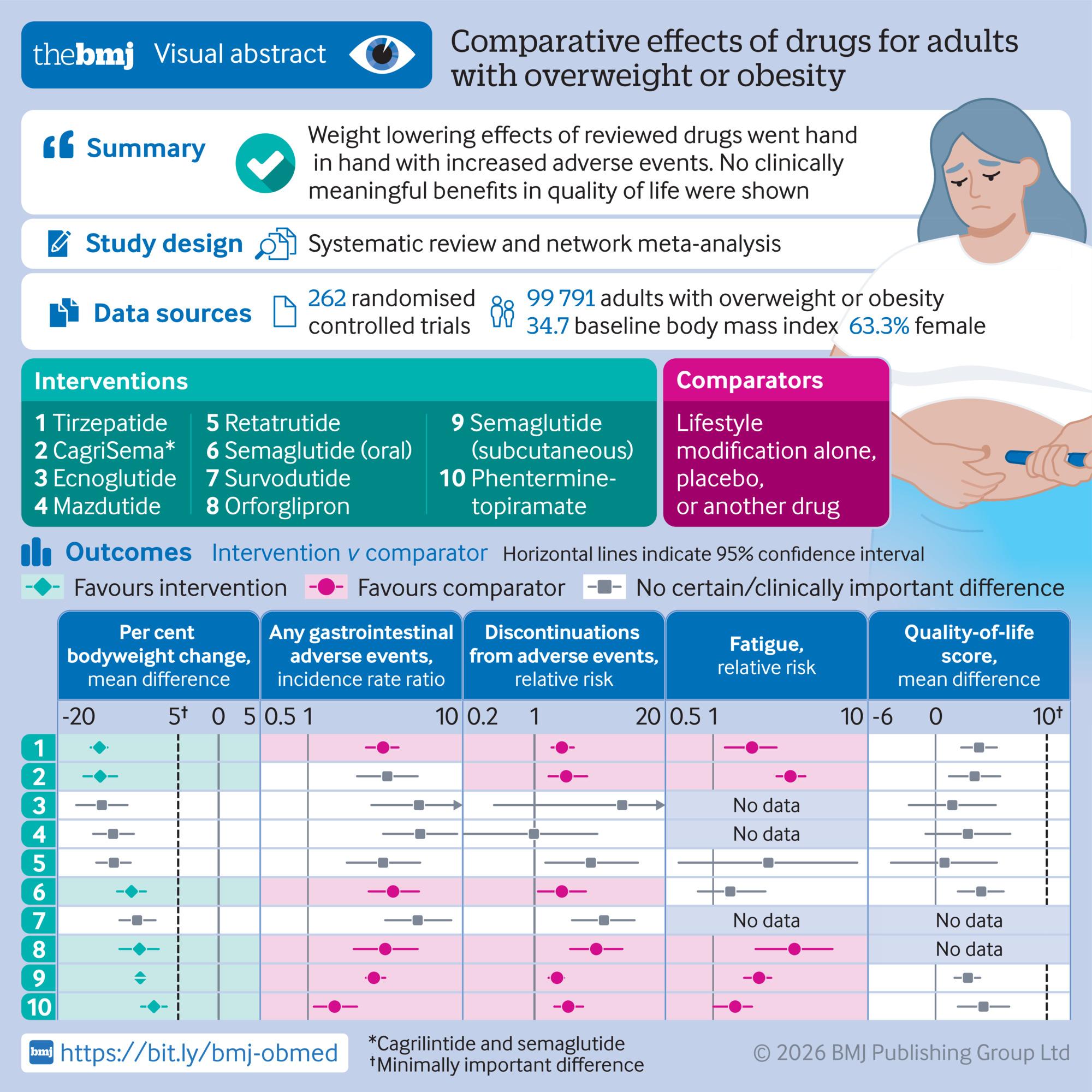
Weight-loss medications such as semaglutide and tirzepatide have moved rapidly from specialist clinics into mainstream culture. They are discussed at dinner tables, in boardrooms and across social media, and they are increasingly shaping how people think about food, health, confidence and mobility. Yet a fresh analysis published in The BMJ offers a cautionary message for stakeholders hoping to interpret the trend too narrowly: weight loss does not automatically translate into better quality of life.
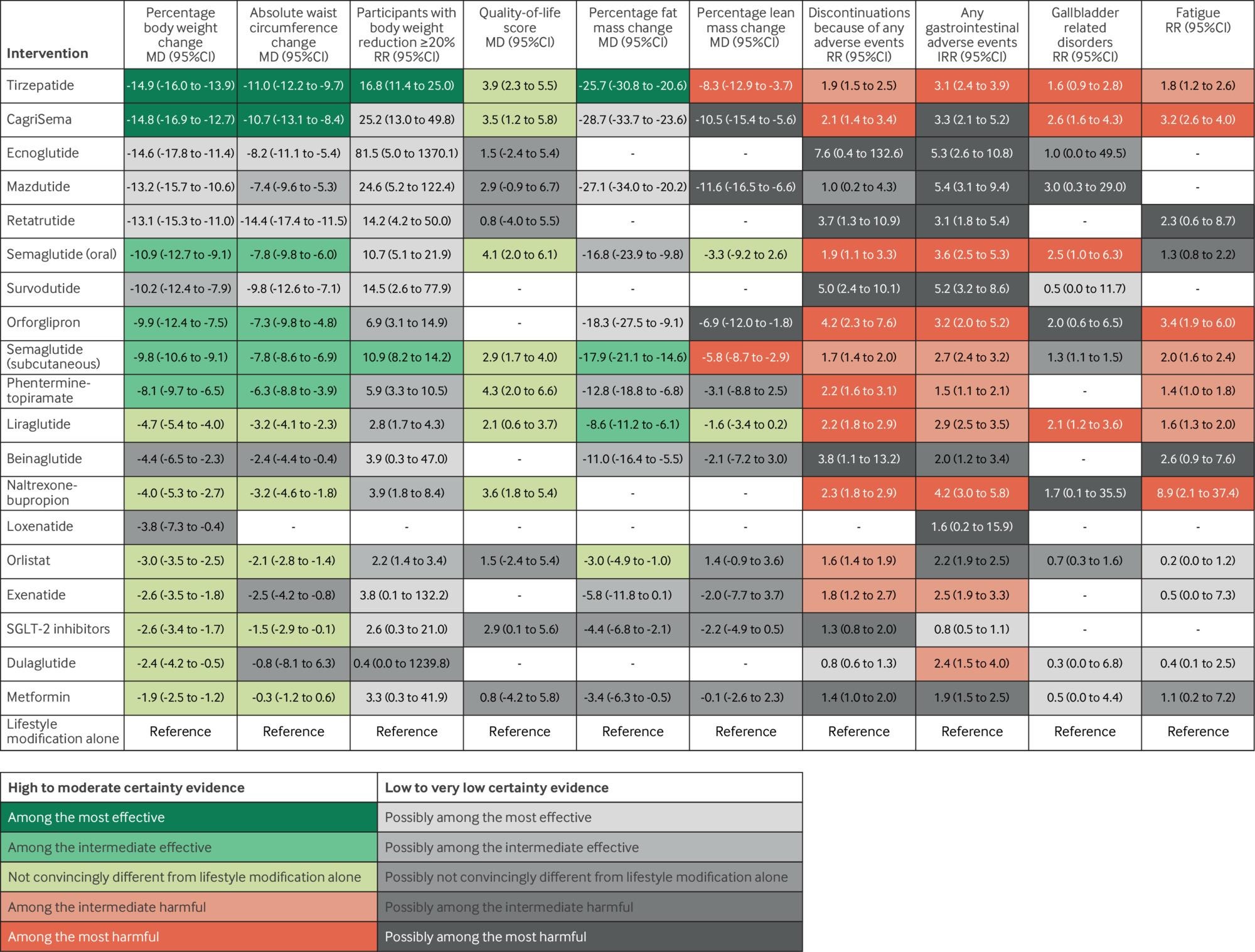
The review assessed 262 randomised trials involving 99,791 participants and 19 obesity drugs. It found that some treatments produced substantial reductions in body weight after one year, led by tirzepatide and CagriSema, but most did not show clinically meaningful improvements in quality-of-life measures. Greater weight loss was also associated with more side effects, higher discontinuation rates and, in some cases, loss of lean mass.
Why this matters for travel
Travel is closely tied to physical comfort, confidence, and perceived freedom of movement. For some travellers using obesity medicines, weight loss may make long-haul flights, walking tours, adventure activities, or resort experiences feel more accessible. Destinations and operators may see growing demand for wellness trips, active holidays, and post-weight-loss lifestyle travel from people who previously avoided certain kinds of journeys.
But the BMJ findings suggest the tourism sector should avoid assuming that pharmacological weight loss equals a straightforward improvement in travel experience. Gastrointestinal side effects, fatigue, treatment burden, and muscle loss can all affect how people plan and enjoy trips. A traveller may lose weight but still need flexible itineraries, rest periods, accessible transport, medical guidance or reassurance around food and medication storage.
Airlines and hospitality may need to rethink comfort, not just capacity
The travel industry has sometimes framed obesity in terms of seat width, passenger weight, and operational costs. The new evidence points to a more human-centred interpretation. If many users do not report meaningful quality-of-life gains after one year, airlines, hotels, cruise operators, and attractions should continue investing in inclusive design rather than assuming medication trends will reduce the need for it.
That means comfortable seating, clear mobility information, non-stigmatising service, flexible dining options, and easy access to medical support remain commercially relevant. GLP-1 use may change some passenger profiles over time, but it does not remove the need to serve travellers with different body sizes, health conditions, and levels of stamina.
A new chapter for medical and wellness tourism
The boom in obesity medicines is also likely to influence medical tourism. Patients already travel for bariatric surgery, cosmetic procedures, and lower-cost care. As GLP-1 access expands, a new category of traveller may emerge, as people seek consultations, prescriptions, follow-up care, or post-weight-loss procedures abroad. Some may look for destinations offering integrated programmes that combine medical oversight, nutrition, exercise, mental wellbeing, and recovery.
However, the study’s findings also underline the risks of marketing weight-loss travel as a quick transformation. Tourism businesses entering this space will need credible clinical partners, transparent pricing, realistic claims, and strong aftercare pathways. Because weight regain after stopping treatment remains a concern, short-term packages that promise lasting change could expose travellers to disappointment and providers to reputational risk.
Food tourism faces subtle shifts
GLP-1 medicines can reduce appetite and alter eating patterns, which may have implications for restaurants, hotels, cruise lines, and gastronomy and food production tours. Some travellers may prefer smaller portions, lighter menus, protein-forward meals, or alcohol-free experiences. Others may want to participate in food culture without overconsumption, making tasting menus, shared plates, and flexible dining formats more attractive.
For destinations known for gastronomy, this does not mean food tourism will decline. Instead, it may become more experiential and less volume-driven. Storytelling, provenance, local producers and sensory experiences could matter more than abundance. The opportunity is to design hospitality that welcomes travellers whose relationship with food is changing without making them feel singled out.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}